Serious burns: definition and characteristics

What is a serious burn?
According to the World Health Organisation (WHO), around 11 million people suffer burns every year and 180,000 die from them(1). In France, serious burns are common, with around 1,000 deaths each year(2).
Burns are the fourth most common type of trauma in the world and a major cause of death and disability in developing countries(3).
Burns occur in a variety of situations: domestic accidents (52%), accidents at work (18%), leisure accidents (10%), attempted suicide (3%), road traffic accidents (3%), fires (3%), etc.(2)
A serious burn is extensive destruction of the skin, damaging its deeper layers and sometimes underlying tissues such as muscles, nerves and even bones. They can be life-threatening.
A burn will be considered serious depending on the depth, the body surface affected, the location of the burned area, the victim's age and underlying systemic diseases and co-morbidities(2,4).
Early treatment of burn victims determines vital prognosis(2).
What is the difference between a minor burn and a serious burn?
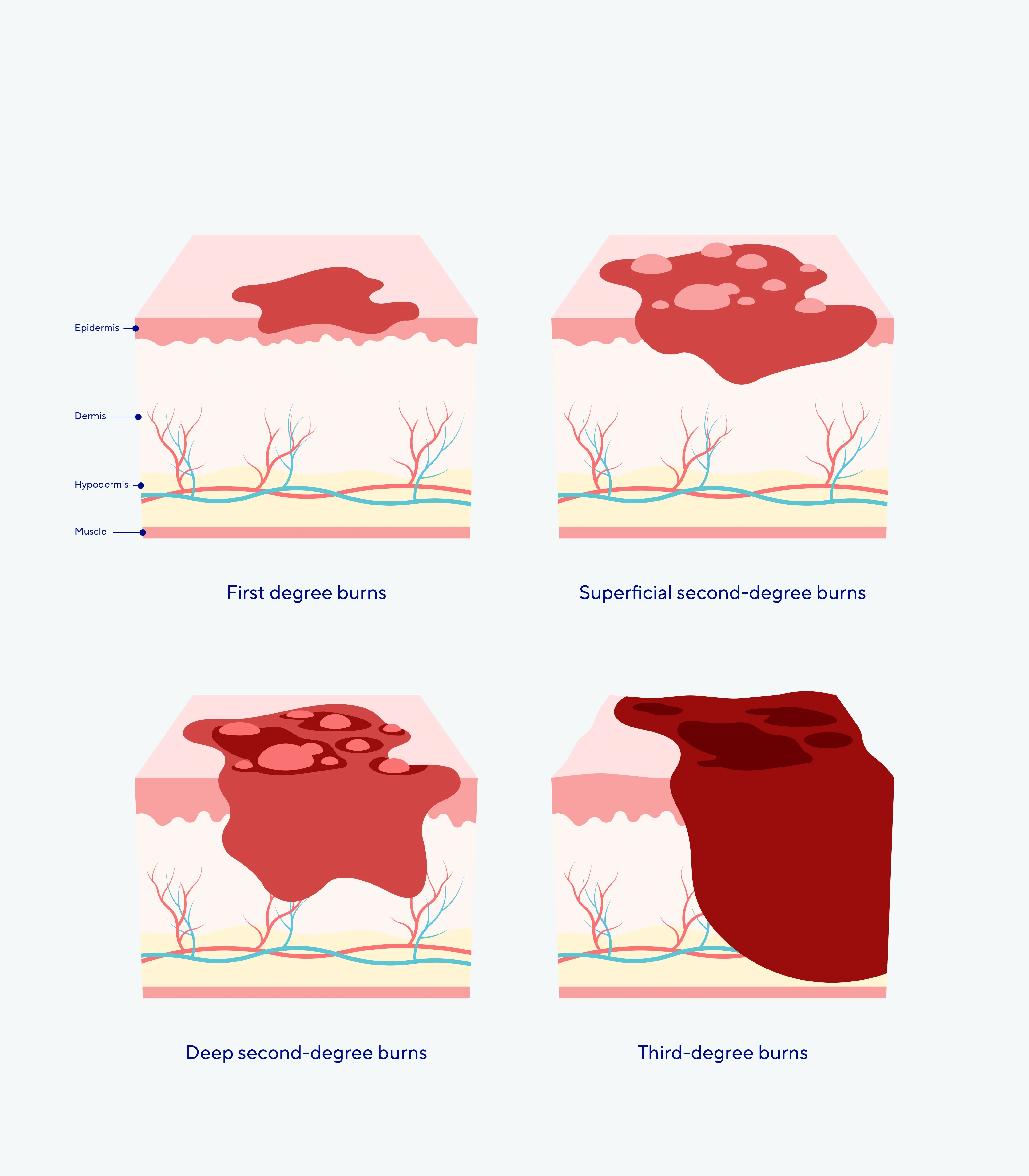
Burns are generally classified according to their location, the extent of the area affected and their degree. There are 3 degrees of burn depending on the depth of the burn: 1st, 2nd or 3rd degree(4,5).
First degree burns: Limited to the epidermis, causing redness and pain without blistering.
Second degree burns: extend to the dermis, blister and are further divided into :
- Superficial second-degree burns: affect the outermost half of the dermis.
- Deep second-degree burns: extend beyond the middle of the dermis.
Third-degree burns: spread over the entire cutaneous layer (epidermis, dermis, hypodermis) and may extend to the underlying tissues. The burn is whitish, charred or brownish, and often insensitive to pain due to the destruction of nerve endings. There are no blisters.
How to recognize burns ?
Superficial burns (first degree and superficial second degree) can heal spontaneously without after-effects, whereas deep burns (deep second degree and third degree) require surgery (excision-grafting) and may be accompanied by functional after-effects. They are therefore considered to be more serious(2).
In terms of extent, a burn is generally estimated as a percentage of the body surface area. Any burn affecting more than 10% of the total skin surface area is considered a serious burn(2).
Calculating the surface area of the skin is therefore essential. To calculate this easily, Wallace's rule of 9 can be used; each area of the body corresponds to a percentage. The palm of a patient's hand, for example, corresponds to 1% of the body surface area(2).
To put it simply, if a burn shows deep destruction or blistering over an area equivalent to more than half the palm of the victim's hand, then the burn is serious.
Localized burns to the face, neck, eyes, nose, hands, natural orifices, genitals or inner thighs and flexion creases (elbow, knee, etc.) are classified as serious burns, even if the extent is limited. Airway burns and circular burns of the limbs are also at risk(2).
In terms of age, burns are more likely to be serious at the extremes of life: in children under the age of 3 and adults over the age of 60(2).
Certain illnesses also worsen the prognosis: heart, respiratory, liver or kidney failure, diabetes, smoking, chronic alcoholism(21).
What are the main causes of serious burns?
Burns can be caused by a variety of sources such as heat, chemicals, electricity, friction or radiation(2,4):
Thermal burns
They are caused by heat sources such as fire, hot liquids or steam. These are the most common (80% of cases).
Chemical burns
They are caused by contact with corrosive or irritating chemical substances, such as acids, bases or toxic products. They are often small but deep.
Electrical burns
They are caused by electrical currents passing through the body, potentially damaging deep tissue. They can more easily lead to serious injury.
Friction burns
They are the result from intense and rapid rubbing of the skin against a rough or abrasive surface, causing both thermal and mechanical damage.
Radiation burns
They are caused by exposure to radiation such as UV rays, X-rays or ionising radiation (such as that emitted by radioactive materials or during medical treatments such as radiotherapy).

Why are severe burns particularly dangerous?
Severe burns can provoke severe systemic responses, i.e. a global and generalised response in the body, which can affect several systems or organs(6,7). This can lead to a series of complications affecting various organ systems and the patient's general condition, such as :
Infections and septicaemia
Infection is the most frequent complication and cause of death in patients suffering from burns. These patients are susceptible to burn wound infection and sepsis(8,9).
Cardiovascular dysfunction
Haemodynamic failure may occur following the burn and may progress to a multivisceral failure syndrome (renal, hepatic...). (2) Burns can cause massive displacement of fluids, which can lead to hypovolaemic shock, meaning that the heart cannot pump enough blood to supply the vital organs with oxygen.
There is also an increase in inflammation and hypermetabolic syndrome, leading to cardiac dysfunction(10).
Respiratory problems
Respiratory distress can occur when inhaling fire fumes(2).
Mental health problems
Serious burns can have a significant impact on mental health, leading to disorders such as depression due to the change in physical appearance, pain, discomfort, the change in appearance, the trauma they may have created, etc.
Healing difficulties
Slow healing, wound infection, pain and hypertrophic scars are a major challenge in the research and management of burns, despite the progress made in treatment and care(11,12).
Mortality and morbidity
The mortality rate in burn patients remains high, with complications such as sepsis and multi-organ dysfunction being important factors(9).
Did you know?
About 11 million
people suffer from burns according to the WHO(1).
180 000
people die from it every year according to the WHO(1).
1 000
deaths every year in France.
4th
Burns are the fourth most common type of trauma worldwide, and a major cause of death and disability in developing countries(3).
Serious burns: what to do?
First aid in the event of a severe burn is essential to minimise the extent of injuries and reduce functional and cosmetic complications and after-effects(13).
The first reaction is to call 15, follow the instructions given and move the victim away from the burning agent (source of the burn) if possible. If the clothing does not adhere, remove it. If they do adhere to the skin, do not remove them, unless they are impregnated with hot liquids or chemicals that deepen the burn(2).
The burn should then be cooled immediately:
Applying running water at room temperature/tide by running until help arrives (minimum 10/15 minutes) reduces the extent of the burn, the pain and considerably reduces the severity, the healing time and the need for skin grafts(2,14,15).
Caution! Although first aid practices vary considerably from one country to another, from one region to another or from one person to another, you must be vigilant about inappropriate or harmful methods such as applying food, oil, shampoo, toothpaste or ice to burns. Only apply water and never puncture blisters.
Serious burns require urgent medical attention and specialist care, often in burns units, because of the risk of complications such as infection, shock and severe scarring.
Choosing your product

 Skin ladderproof glove Cicatrex - Open-finger short sleevelet (wrist)Skin ladderproof glove Cicatrex - Open-finger short sleevelet (wrist)
Skin ladderproof glove Cicatrex - Open-finger short sleevelet (wrist)Skin ladderproof glove Cicatrex - Open-finger short sleevelet (wrist)Medical compression glove














- Radzikowska-Büchner E, Łopuszyńska I, Flieger W, Tobiasz M, Maciejewski R, Flieger J. An Overview of Recent Developments in the Management of Burn Injuries. Int J Mol Sci. 2023 Nov 15;24(22):16357. doi: 10.3390/ijms242216357. PMID: 38003548; PMCID: PMC10671630.
- CEMIR Collège des Enseignants de Médecine Intensive - Réanimation , Médecine intensive, réanimation, urgences et défaillances viscérales aigues, 7ème édition, Elsevier Masson
- Odondi, R., Shitsinzi, R., & Emarah, A. (2020). Clinical patterns and early outcomes of burn injuries in patients admitted at the Moi Teaching and Referral Hospital in Eldoret, Western Kenya. Heliyon, 6. https://doi.org/10.1016/j.heliyon.2020.e03629.
- Burgess, M., Valdera, F., Varon, D., Kankuri, E., & Nuutila, K. (2022). The Immune and Regenerative Response to Burn Injury. Cells, 11. https://doi.org/10.3390/cells11193073.
- Abraham, J., Plourde, B., Vallez, L., & Nelson-Cheeseman, B. (2016). Correcting a prevalent misunderstanding of burns.. Burns : journal of the International Society for Burn Injuries, 42 4, 715-6 . https://doi.org/10.1016/j.burns.2016.01.003.
- Burgess M, Valdera F, Varon D, Kankuri E, Nuutila K. The Immune and Regenerative Response to Burn Injury. Cells. 2022 Sep 29;11(19):3073. doi: 10.3390/cells11193073. PMID: 36231034; PMCID: PMC9563909.
- Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers. 2020 Feb 13;6(1):11. doi: 10.1038/s41572-020-0145-5. PMID: 32054846; PMCID: PMC7224101.
- D'Abbondanza JA, Shahrokhi S. Burn Infection and Burn Sepsis. Surg Infect (Larchmt). 2021 Feb;22(1):58-64. doi: 10.1089/sur.2020.102. Epub 2020 May 4. PMID: 32364824.
- Zhang, P., Zou, B., Liou, Y., & Huang, C. (2021). The pathogenesis and diagnosis of sepsis post burn injury. Burns & Trauma, 9. https://doi.org/10.1093/burnst/tkaa047.
- Tapking, C., Popp, D., Herndon, D., Branski, L., Hundeshagen, G., Armenta, A., Busch, M., Most, P., & Kinsky, M. (2020). Cardiac Dysfunction in Severely Burned Patients: Current Understanding of Etiology, Pathophysiology and Treatment.. Shock. https://doi.org/10.1097/SHK.0000000000001465.
- Markiewicz-Gospodarek, A., Kozioł, M., Tobiasz, M., Baj, J., Radzikowska-Büchner, E., & Przekora, A. (2022). Burn Wound Healing: Clinical Complications, Medical Care, Treatment, and Dressing Types: The Current State of Knowledge for Clinical Practice. International Journal of Environmental Research and Public Health, 19. https://doi.org/10.3390/ijerph19031338.
- Wang, Y., Beekman, J., Hew, J., Jackson, S., Issler-Fisher, A., Parungao, R., Lajevardi, S., Li, Z., & Maitz, P. (2018). Burn injury: Challenges and advances in burn wound healing, infection, pain and scarring. Advanced Drug Delivery Reviews, 123, 3–17. https://doi.org/10.1016/j.addr.2017.09.018.
- Leon-Villapolas, J. (2019). Burns first aid. Burns (OSH Surgery). https://doi.org/10.1093/MED/9780199699537.003.0008.
- Palmieri, T. (2023). Acute care for burn patients: fluids, surgery, and what else?. Current Opinion in Critical Care, 29, 696 - 701. https://doi.org/10.1097/MCC.0000000000001096.
- Harish, V., Tiwari, N., Fisher, O., Li, Z., & Maitz, P. (2019). First aid improves clinical outcomes in burn injuries: Evidence from a cohort study of 4918 patients.. Burns : journal of the International Society for Burn Injuries, 45 2, 433-439 . https://doi.org/10.1016/j.burns.2018.09.024.